Mitigation of Air Pollution and its Impact on the Lung Health of Tuberculosis Patients, a Prospective Cohort Study from Rural India
Ajay Kumar Singh1
 , Satish Kumar Bhardwaj2
, Rajeev Kumar Aggarwal2
*
, Dimple Kumar Bhaglani3
, Amit Guleria4
, Kartikey Sahil2
, Gagan Deep Raj Hans1
and Meenu Saini5
, Satish Kumar Bhardwaj2
, Rajeev Kumar Aggarwal2
*
, Dimple Kumar Bhaglani3
, Amit Guleria4
, Kartikey Sahil2
, Gagan Deep Raj Hans1
and Meenu Saini5
1
Department of Health and Family Welfare,
District Programme Officer,
Solan,
Himachal Pradesh
India
2
Department of Environmental Science,
College of Forestry, YS Parmar University of Horticulture and Forestry,
Nauni, Solan,
Himachal Pradesh
India
3
Department of Pulmonary Medicine,
IGMC,
Shimla,
Himachal Pradesh
India
4
Department of Economics and Sociology,
College of Basic Sciences and Humanities, Punjab Agricultural University,
Ludhiana,
Panjab
India
5
Department of AYUSH,
Ayurvedic Medical Officer,
Mehendobag, Sirmour,
Himachal Pradesh
India
http://dx.doi.org/10.12944/CWE.19.3.18
Copy the following to cite this article:
Singh A. K, Bhardwaj S. K, Aggarwal R. K, Bhaglani D. K, Guleria A, Sahil K, Hans G. D. R, Saini M. Mitigation of Air Pollution and its Impact on the Lung Health of Tuberculosis Patients, a Prospective Cohort Study from Rural India. Curr World Environ 2024;19(3). DOI:http://dx.doi.org/10.12944/CWE.19.3.18
Copy the following to cite this URL:
Singh A. K, Bhardwaj S. K, Aggarwal R. K, Bhaglani D. K, Guleria A, Sahil K, Hans G. D. R, Saini M. Mitigation of Air Pollution and its Impact on the Lung Health of Tuberculosis Patients, a Prospective Cohort Study from Rural India. Curr World Environ 2024;19(3).
Download article (pdf)
Citation Manager
Publish History

Introduction
Globally, polluted air is the largest environmental health risk factor leading to respiratory diseases, both obstructive and restrictive in nature. Every year 4.3 and 3.7 million people die across the world due to polluted ambient and indoor air respectively1. Tuberculosis (TB) is the world’s second leading cause of death from a single infectious agent2. India ranks amongst the six countries which share 60 % of the global burden of the disease3. Henceforth, the elimination of the disease from the world largely depends on the preventive and curative care adopted in the country4, 5. Gasses such as O3, NO2, SO2, VOC, CO and other pollutants such as particulate matter enhance the susceptibility of the lung parenchyma to tuberculosis development6, 7.
Maintaining ambient air quality by ameliorating environmental determinants has been reported to improve respiratory health and decrease in the incidence of TB infection8. Whereas, ambient and indoor air pollution may lead to millions of deaths annually across the world9.
Numerous case studies, ecological analysis and animal experiments have evinced that the pollutants such as PM2.5 and PM10, gases such as O3, NO2, SO2, VOC, and CO may alter the functions of macrophages by decreasing the interferon-gamma and tumour necrosis factor levels, may lead to decreased immunity and increased chances of developing the tubercular disease. The poor air quality has been reported to result in decreased lung compliance as indicated by total lung capacity, inspiration capacity, expiratory reserve volume and residual volume. Therefore, the present study was undertaken to work out ways to end the TB epidemic to achieve the Sustainable Development Goals globally10 and the WHO targets to decrease TB incidences by 80% by the end of 2030 in comparison to 201511. Scientific experts have emphasised adopting a holistic approach to eliminating tuberculosis by educating different stakeholders and incorporating the promotive, preventive and curative sciences12,-14.
Under the domain of the Stop TB strategy, the vulnerable population is being protected from developing TB. Persons living in polluted air areas (both rural and urban) are a vulnerable group. In India, 68.84% of the population lives in rural areas, mostly villages15 and there is a scarcity of healthcare facilities in the countryside regions16. Moreover, social stigma and taboos associated with TB still exist in these rural settings of Indian society and here it is a neglected disease17. Therefore, the present study was undertaken to assess the relationship between the air quality and the lung health of Tb patients along with an assessment of the effect of air pollution mitigation on the air quality index (AQI).
Materials and methods
Study Design
A prospective cohort interventional study was undertaken.
Study Population
The study participants were the pulmonary tubercular patients diagnosed in the Designated Microscopy Centre (DMC) of the secondary care hospital of the district, Regional Hospital Solan and the residents of those villages to which the diagnosed tubercular patients belonged.
Study Area
The awareness camps and air quality assessments were undertaken in the ten villages of Solan, an industrializing region in northern India.
Study period: The study was conducted during the years 2018-2020. The assessments of air quality, lung health, knowledge and practice attributes of participants were undertaken during the years 2018-2019.
Sample Size
To achieve the objectives twenty-three diagnosed tubercular patients, residents of ten villages of Solan district of HP were enrolled in the study (Figure 1).
 | Figure 1: Map of the Study Area
|
Inclusion Criteria
The study group included all those TB patients who successfully completed the anti-tuberculosis treatment regimen in 2018, for drug-sensitive TB, for six months and did not consume any medicine other than that of anti-TB drugs.
The study also included the first 30 villagers (age > 18 years) who gave voluntary consent for participation in the study, from each of the 10 resident villages (N=300) of the TB patients.
Baseline knowledge and practice attributes about the environmental determinants and mitigation of air pollution were assessed for these 300 villagers at the beginning of the study by using a pilot-tested standardized questionnaire. Awareness camps for the mitigation of air pollution were organized for these study participants. Simultaneously, the baseline lung volume status of the diagnosed tubercular patients (N=23) was also measured at the start of anti-tubercular treatment. The Lung Health Index was calculated. The baseline ambient AQI of these 10 villages was also calculated.
Awareness camps were organized in the selected villages for enrolled participants (N=300) at the time of the start of the anti-tubercular treatment of the selected TB patients.
The following intervention steps were taught to the study participants (N=300) by means of awareness camps:
Adoption of scientific waste disposal methods and avoiding improper, unscientific waste disposal.
Stopping littering around the residential regions.
Not following stubble burning by farmers, advocating burial methods for stubble disposal.
Avoiding waste burning in the region, adopting scientific waste disposal.
Stopping indoor mud cook stove burning and usage of liquefied petroleum gas (LPG) as fuel for cooking alternatively.
Industries if any in the village, to monitor and ameliorate all the untreated industrial emissions.
Adoption of cross-ventilations in residential and industrial premises.
Adopting various architectural changes to ensure cross ventilation.
Adoption of air pollution abating plants (indoor and outdoor)
The respondents were encouraged to grow the following pollution-abating plants inside their housing settings and outdoor as well:
Indoor Plants
Justiciaadhatoda (Basuti), Murrayakoenigii (Kadipatta), Catharanthusroseus (Chinesesadabahar), Spathiphyllumwallissi (Peace lily), Chamaedoreaseifrizii (Bamboo palm), Rhapisexcelsa(Rafiz palm), Philodendron scandens(Philodendron), Ficuselastica(Rubber plant), Dypsislutescens (Areca palm), Ficusbenjamina(Weeping fig), Salvarosmarinus(Rosemary), Dracaena trifasciata (Snake plant), Gerbera jamesonii(Gerbera jedi), Dendrathemagrandiflora(Guldaodi), Hedera helix(English ivy) and Aloe vera (Aloe-vera), Epipremnumaureum (Golden pothos), Tabernaemontanadivaricata (Chandni) and Chlorophytumcomosum (Spider plant).
Outdoor Plants
Jasminumgrandiflorum (White chameli), Ficusreligiosa(Peepal), Terminaliabellerica(Bajeda),Bauhinia variegata (Kachnaar), Syzygiumcuminii(Jamun), Cassia fistula(Amaltaas), Emblicaofficinalis(Amla), Azadirachtaindica(Neem), Ficusbenghalensis (Bargad), Millettiapinnata(Karanj), Cascabelathevetia(Peetkaner), Cestrum nocturnum(Raatki rani), Terminaliaarjuna (Arjun) and Jatrophacuracas(Jetropa),
To determine the impacts, the knowledge and practice attributes about air pollution mitigation were again assessed after a span of six months. Lung volumes were also repeated by spirometry and Lung Health Indices. AQI of the of the selected housing settings was computed by measuring all its indicators.
Pilot pilot-tested standardized questionnaire (Interviewer administered) was employed to elicit knowledge and practice attributes of the rural population about maintaining good air quality indoors as well as outdoors.
Calculation of AQI
Ambient air quality assessment by monitoring four important criteria of air pollutants was conducted in the selected ten villages by employing a Respirable Dust Sampler (Cat. No MBLRDS-002) and Fine Dust Sampler (DFPM 2.5 SAMPLER). The samplers were employed for two days at each of the ten sites. Further analysis was done by gravimetric (particulate matter) and volumetric (gaseous pollutants) methods18
Method for analysis of Air Quality Index
The AQI was calculated from the observed NO2, SO2, PM10 and VOC, values by using the following formulae19:

Where:
IPM, ISO2, INOX and Ivoc in equation (1) are individual values of particulate matter, sulphur dioxide, oxides of nitrogen and volatile organic compounds, respectively. SPM10, SSO2, SNOX and Svoc are standards of ambient air quality with concentration values in ambient air (µg/m3) as 100, 60, 80 and 80 respectively.
Statistical Analysis Plan
Principal Component Analysis (PCA) was used for the analysis of the following parameters among the study participants (N=300):
Knowledge of eight factors determining the quality of the environment like scientific waste disposal, littering, stubble burning, waste burning, etc.
Adoption and practicing the eight methods which ameliorate the environment by mitigation of air pollution.
Under the method PCA, principal components were derived such that their number was equal to the number of determinants of the environment. Principal component 1 (PC 1) carried the highest variation among all the principal components. Henceforth, PC 1 was employed to assign the weight for each environmental determinant.
![]()
Where b denoted each component’s coefficient.
The weights were calculated as the proportion of the coefficient of each parameter in equation (1) in such a manner that the sum of the weights equalled to 1.
The next step involved the process of standardization of parameters which was achieved by using the formulae:
Actual value - minimum value / maximum value – minimum value
Each individual/village index values were then calculated as
![]()
Where x1n denoted the standardized values of the nth parameter of individual/village 1 and wn represented the weight of the nth parameter calculated by PCA.
It was assumed that value 1 of the principal knowledge index inferred no knowledge and value 0 as high knowledge. For the principal practice index, the values 1 and 0 referred to not practicing and practicing the environmental amelioration steps respectively.
Thereafter, all the index values were calculated i.e., the principal knowledge index and the principal practice index were computed using methods of simple linear regression and two-way ANOVA by using Statistical Package for Social Sciences (SPSS), version-21 software.
Results and Discussion
The mean age of the tubercular patients (N=23; males = 46.7%; females = 53.3%) was 26.58 ± 6.89 years. 68.9% of patients were from rural and 31.1% from urban areas. 88.9% were employed and only 2.2% of the patients had education below the primary level of education i.e. fifth standard. 28.9% had an education level between the primary and secondary level of school education. The majority of the patients were graduates (68.9%).
The principal knowledge index was calculated for every 30 participants selected out of 10 villages of the Solan district of HP. In total, there were 300 respondents (N=300) from five villages each in the year 2018 and 2019 respectively. This was calculated before and after the organization of the environment amelioration awareness camp (Supplementary Tables 1 and 2). The average principal knowledge index ranged from 0.59 in village number 3 to 0.82 in village number 7 before the organization of the camps whereas it varied from 0.08 in village number 7 to 0.19 in village number 6 after the camps.
Similarly, the Principal Practice index was calculated. Supplementary Tables 3 and 4 depicted the values of all the respondents before and after the organization of camps. It was from 0.52 in village number 4 to 0.70 in village number 8 before the camps and from 0.14 in village number 3,4,5 and 6 to 0.70 in village number 8.
Analysis by Two-way ANOVA inferred (Table 1) that the highest knowledge (0.08) was observed in village 7 during the post-camp period. The knowledge about the eight environmental parameters varied significantly with the pre- and post-organization of the awareness programmes amongst the villagers. The highest knowledge (0.14) was observed post the organization of the camps (values being closer to 0, which we had assumed as inferring: having the knowledge). This was in comparison to low knowledge (0.73) prevailing before the organization of the camp (value closer to 1, which we had assumed that 1 inferred having no knowledge).
The study also evinced that during the post-camp period i.e. after six months of the organization of sensitization camps, the practice of adopting the environmental ameliorating steps of mitigating air pollution was more by the village residents (0.17, which is closer value to 0 and we had assumed 0 as the presence of the practice of the environmental parameters).
Table 1: Two-way analysis of variance of knowledge and practice about environmental ameliorative parameters in the rural settings of Solan District of HP
Parameter | Individual parameter weight | Village No. | Knowledge Index | Practice Index | ||||
Pre-training | Post-training | Mean | Pre-training | Post-training | Mean | |||
a. Scientific waste disposal | 0.12 | 1 | 0.12 | 0.44 | 0.63 | 0.19 | 0.41 | 0.30 |
b. Harmful health effects of littering | 0.14 | 2 | 0.75 | 0.11 | 0.43 | 0.57 | 0.17 | 0.37 |
c. Harmful health effects due to stubble burning | 0.14 | 3 | 0.59 | 0.17 | 0.38 | 0.64 | 0.14 | 0.39 |
d. Harmful health effects of waste burning | 0.14 | 4 | 0.71 | 0.18 | 0.44 | 0.52 | 0.14 | 0.33 |
e. Harmful health effects of indoor mud cookstove burning | 0.12 | 5 | 0.77 | 0.17 | 0.47 | 0.59 | 0.14 | 0.36 |
f. Harmful health effects of untreated industrial emission | 0.09 | 6 | 0.78 | 0.19 | 0.48 | 0.62 | 0.14 | 0.38 |
g. Knowledge of indoor cross- ventilation | 0.12 | 7 | 0.82 | 0.08 | 0.45 | 0.64 | 0.15 | 0.40 |
h. Harmful health effects of waste burning | 0.13 | 9 | 0.73 | 0.11 | 0.42 | 0.62 | 0.19 | 0.41 |
i. Harmful health effects of indoor mud cook-stove burning | 0.11 | 10 | 0.68 | 0.14 | 0.41 | 0.62 | 0.19 | 0.40 |
Mean | 0.73 | 0.14 | 0.62 | 0.17 | ||||
CD Camp Villagex Camp Village | 0.03 0.07 0.13 | 0.04 0.09 0.13 | ||||||
The individual weights of the four different types of lung volumes of the study participants were calculated. Thereafter respective individual principal components were calculated by the PCA statistics (Table 2).
Table 2: Principal component values of the four lung volumes
Parameter | Individual parameter weight | Principal component value | |||
FVC | 0.11 | 0.84 | 0.20 | 0.48 | |
FEVI | 0.62 | 0.62 | 0.19 | 0.40 | -0.65 |
Ratio | 0.52 | 0.52 | -0.49 | 0.38 | 0.58 |
PEFR | 0.58 | 0.58 | 0.07 | -0.81 | 0.08 |
Table 3 depicted the lung volumes of the study participants during pre- and post-organisation of awareness camps. The table also illustrates the overall principal lung volume index. During the pre-organization of the camps, the principal lung volume index ranged from 0.36 in the village no 3 to 0.73 in the village no 2. The index also varied from 0.25 in village number 4 to 0.73 in village no 1.
Table 3 Effects of awareness programmes on lung volumes in rural settings of Solan district of HP
Village No. | FVC | FEV1 | Ratio | PEFR | Principal Lung Volume Index | |||||
Pre-camp | Post-camp | Pre-camp | Post-camp | Pre-camp | Post-camp | Pre-camp | Post-camp | Pre-camp | Post-camp | |
1 | 70.50 | 76.00 | 77.50 | 87.00 | 111.00 | 114.00 | 39.50 | 48.50 | 0.64 | 0.73 |
2 | 102.00 | 120.00 | 101.00 | 87.50 | 100.00 | 73.50 | 45.00 | 37.50 | 0.73 | 0.58 |
3 | 82.00 | 84.00 | 51.00 | 58.50 | 61.50 | 69.00 | 26.00 | 27.00 | 0.36 | 0.41 |
4 | 107.00 | 81.00 | 107.00 | 42.00 | 100.00 | 52.00 | 34.00 | 17.00 | 0.68 | 0.25 |
5 | 79.50 | 106.00 | 61.50 | 65.00 | 77.00 | 62.00 | 34.50 | 39.00 | 0.48 | 0.49 |
6 | 78.50 | 91.50 | 68.00 | 76.50 | 87.00 | 81.00 | 29.50 | 31.00 | 0.49 | 0.52 |
7 | 67.33 | 102.67 | 70.00 | 73.17 | 101.67 | 76.00 | 35.83 | 31.00 | 0.57 | 0.50 |
8 | 66.33 | 104.67 | 67.67 | 87.67 | 103.00 | 83.33 | 29.33 | 35.00 | 0.53 | 0.59 |
9 | 59.00 | 75.00 | 63.00 | 72.00 | 107.00 | 97.00 | 28.00 | 27.00 | 0.51 | 0.51 |
10 | 75.50 | 114.50 | 87.00 | 59.50 | 116.50 | 45.00 | 34.50 | 40.50 | 0.66 | 0.44 |
Mean | 78.77 | 95.53 | 75.37 | 70.88 | 96.47 | 75.28 | 33.61 | 33.35 | 0.56 | 0.50 |
± Std Dev | ±15.29 | ±16.21 | ± 17.88 | ± 14.93 | ± 16.70 | ± 20.40 | ± 5.73 | ± 8.77 | ±0.11 | ± 0.12 |
Regression Statistics Analysis
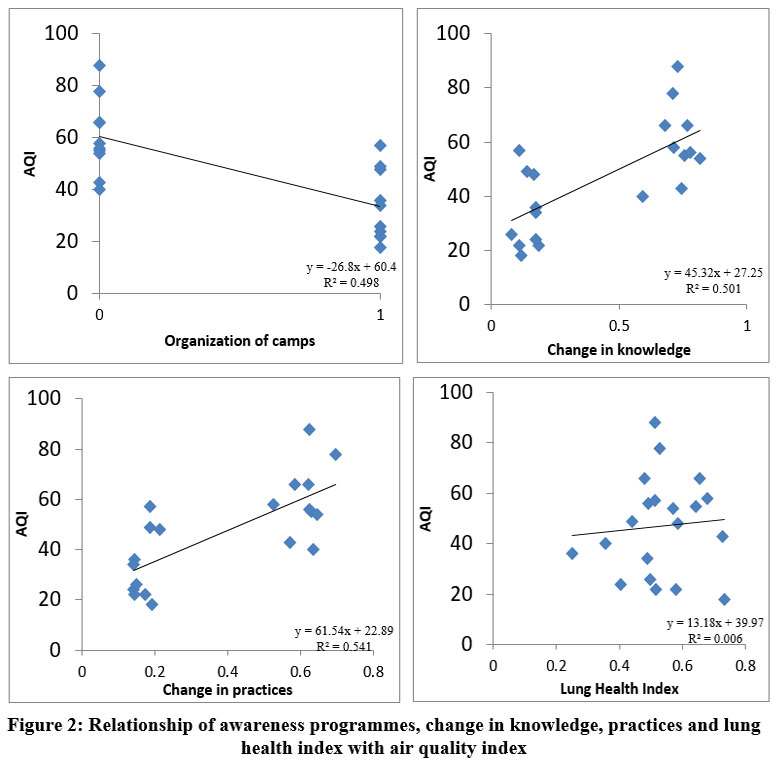 | Figure 2: Relationship of awareness programmes, change in knowledge, practices and lung health index with air quality index
|
The air quality index of the villages improved significantly (p<0.05) after the people were made educated regarding the role of air quality and its relationship with human health. The AQI had dropped by 26.8 units after the six months of interventions taken up by village administrative bodies as trained. The improvement in air quality through education and amelioration of indoor air quality by introducing pollution-abating plants has also been reported17, 20.
The increase in the knowledge of rural people was noticed to improve the AQI. Significant improvement of AQI by about 45.32 units may be attributed to increased literacy of the rural people with respect to air quality and its management. AQI improved by 61.55 units with the adoption of practices like enhancing air circulation in the housing settings and growing pollution-abating plants on the premises and indoors as well as outdoors. Although there was no significant effect observed in the lung health index in relation to the changes observed in the AQI, there was a per unit increase in the lung health index with 0.0005 units improvement in Air Quality and lung health index by 0.06 with the per unit of training organised. A positive correlation (r = 0.31) was inferred between the organization of the awareness camps and AQI improvement. A positive correlation, although mild, has also been observed similarly between the improvement in the knowledge base and air quality (r = 0.25). Lung health improvement showed a positive correlation (r = 0.17) with the improved AQI and the awareness created (r = 0.25). The results are in line with the findings which have also advocated a positive relationship between the awareness level of the community about air quality and its impact on human health21, 22. Further, they have also indicated the positive influence of air quality improvement on human health. Similarly, another study also demonstrated the positive effect of air quality improvement on lung health maintenance23. The importance of creating literacy among people on air quality maintenance and environmental amelioration in the management of tuberculosis has also been highlighted by the World Health Organization24. The need for environmental parameter assessment had been similarly studied by Sharama and Dikshit in 201225.
Conclusion
Exposure to PM10, SO2 or NO2 in the long term in indoor and outdoor environments is associated with increased odds of tuberculosis. It is evident that better air quality at both indoor and outdoor levels may ease the burden of this disease. Maintaining air quality through capacity building of tuberculosis patients on various management options proved effective in improving ambient and indoor air quality in rural settings vis a vis tuberculosis patient’s health in the Solan district of HP. In rural areas, introduction of pollution-abating plants indoors and outdoors along with the improvement of ventilation in housing settings improved the air quality index and overall respiratory health of the tubercular patients. The enhanced knowledge of the patients regarding the significance of the air quality in tuberculosis management especially in rural settings of mountain regions may help in the sustainable management of the disease and will contribute to achieving the sustainable development goal four at the global level. Therefore. findings need to be replicated in other parts to eliminate the TB disease by putting more efforts on enhancing the knowledge base of the rural people.
Acknowledgment
We are grateful to the Department of Environmental Science and Technology, Shimla, H.P., India, for providing the funding support for this study.
Funding Sources
Department of Environmental Science and Technology, Shimla, H.P. No. Env. S&T (F)/ R& D Project/2017-4655 dated 12 February, 2018
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
The manuscript incorporates all data sets produced or examined Throughout this research study
Ethics Statement
Institutional ethics committee permission was secured from the YS Parmar University of Horticulture and Forestry vide No. Env. S&T (F)/ R&D Project/2017-4655 dated 12 February, 2018.
Informed Consent Statement
Informed written consent was obtained from the study participants i.e. the tuberculosis patients, the village residents who attended the awareness camps and those household Heads where air quality was measured. Voluntary participation of all study incumbents was ensured.
Authors’ Contribution
Ajay Kumar Singh and Satish Kumar Bhardwaj: Study conception and Design
Ajay Kumar Singh and Rajeev Kumar Aggarwal: Data collection
Amit Guleria and Ajay Kumar Singh: Analysis
Gagan Deep Raj Hans, Dimple Kumar Bhaglani: Interpretation of results
Kartikey Sahil, Meenu Saini and Ajay Kumar Singh: Manuscript preparation
References
- WHO. Compendium of WHO and other UN guidance on health and environment. Geneva: WHO; 2021 (WHO/HEP/ECH/EHD/21.02). Licence: CC BY- NC-SA 3.0 IGO. Available from https://who.int/publications/i/item/WHO-HEP-ECH-EHD. [Last accessed on 2022 March 7].
- WHO. Global tuberculosis report 2023. Geneva: WHO; 2023. Licence: CC BY-NC-SA 3.0 IGO. Available from https://apps.who.int/iris/handle/10665/274453. [Last accessed on 2024 August 15].
- Singh N, Gupta D. Revised National Tuberculosis Control Programme (RNTCP) in India; current status and challenges. Lung India2005;22:107-111.
- Singh A. K, Vadini V, Shridhar P. K, Singh B, Kumari V. Gap analysis of tubercular suspect referrals to a diagnostic microscopy centre in a northern state of India. Int. J. Sci. Res 2019;8(3):67-68.
- S.K. Ajay, C. Sumit, B.K. Dimple, C. Bharti. A cross-sectional study to assess the Tuberculosis Treatment Providers in the mid hills of India. IJTB2018;65:290-95.
CrossRef - Flad H, Gercken J, Hübner L, Schlüter C, Pryjma J, Ernst M. Cytokines in mycobacterial infections: in vitro and ex vivo studies. Arch ImmunolTherExp (Warsz)1995;43:153–158.
- Brunekreef B, Beelen R, Hoek G, Schouten L, Bausch- Goldbohm S, Fischer P, et al. Effects of long term exposure on respiratory and cardiovascular mortality in the Netherlands: the NLCS-AIR Study. Res Rep Health EffInst2009Mar;(139):5–71; discussion 73-89.
- Ranade S. Natural healing through Ayurveda. MotilalBanarasidass, New Delhi; 1999. p. 32.
- WHO. Global tuberculosis report 2015. Geneva: World Health Organization; 2015. Available from: apps.who.int/iris/bitstream/10665/19102/1/9789241565059_eng.pdf. [Last accessed on 2017 March 1].
- UNDP. Sustainable Development. United Nations Development Programme. NewYork:2015. Available from: www.undp.org/content/undp/en/home/sustainable-development- goals.html. [Last accessed on 2017 March 7].
- WHO. The Stop TB Strategy. 2017. Available from: www.who.int/tb/strategy/stop_tb_strategy/en/. [Last accessed on 2017 May 4].
- Samal J. Ayurvedic management of pulmonary tuberculosis: A systematic review. J Complement Med Res2016;5:86-91.
CrossRef - Singh A. K, Bhaglani D. K, R Kumar, V Kumari, Chawla S. A public-private mix intervention to enhance tuberculosis case finding in resource constrained industrial settings. Int. J. Curr. Res2018;10(5):68874-68878.
- Thakur Y, Aggarwal R. K, Bhardwaj S. K, Singh A. Impact of wood burning and mud-cookstove on indoor air quality vis- a- vis human health in Western Himalayan region. SSRG- IJAES2017;4(4):10-15.
CrossRef - Jaiswal A, Singh V, Ogden J. A, Porter J.D. H, Sharma P. P, Sarin R, et al. Adherence to tuberculosis treatment: lessons from the urban setting of Delhi, India. TM & IH.2003;8:625-633.
CrossRef - Singh A. K, Shridhar P. K, Kumar R, Kumari V, Singh B, Bhaglani D. K. Complimenting tuberculosis treatment by Yogic exercises. IJMSIR. 2019;4(4):147-153.
- Singh A. K, Vadini V, Shridhar P. K, Singh B, Bhaglani D. K, Kumari V. Village administration eliciting tuberculosis cases- an innovative approach. Int. J. Recent Sci. Res. 2018;9(12):29942-29945.
- Mukunda R.P. V, Hima B. V, Sagareshwar G, Jayakumar I, Anjaneyulu Y. Assessment of ambient air quality in the rapidly industrially growing Hyderabad urban environment. Workshop program and presentation, air quality monitoring and management, better air quality (BAQ) Conference, Hyderabad, India 2003: 69p.
- Sahil K, Aggarwal R. K, Bhardwaj S. K. Air quality status in fast developing city of Western Himalayan State of India. Clim Change 2016;2(8):573-578.
- Kamineni V. V, Turk T, Wilson N, Satyanarayana S, Chauhan L. S. A rapid assessment and response approach to review and enhance Advocacy, Communication and Social Mobilization for tuberculosis control in Odishastate, India. BMC Public Health2011;11:463.
CrossRef - Nair V. M. Multi-Purpose Health Workers in Primary Health Care; an inter-district sub centre-based study from Kerela, India. MPH. Dissertation. AchuthaMenon Centre for Health Science Studies, SreeChitraTirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerela, India 1998: 82p.
- Ramirez A. S, Ramondt S, Bogart K. V, Zuniga R. P. Public awareness of air pollution and health threats: challenges and opportunities for communication strategies to improve environmental health literacy. J Health Commun2019;24(1): 75-83.
CrossRef - Schraufnagel D. E, Balmes J. R, Matteis S. D, Hoffman B, Kim W. J, Padilla R. P, Rice M, Sood A, Vanker A, Wuebbles D. J. Health benefits of Air Pollution reduction. Ann Am ThoracSoc2019;16(12):1478-1487.
CrossRef - World Health Organization. Millennium Development Goals 2000. [cited 2018 December 2] Available from: URL: www.who.int/topics/millennium_development_goals/en/.
- Sharma M, Dikshit O. Environmental pollution sources and their apportionment to ambient environment: a GIS based study of Solan district. A preliminary report submitted to Himachal Pradesh State Pollution Control Board, New Shimla 2012; pp 41.








