Assessment of Respiratory Morbidity and Epidemiological Survey of Tobacco Smokers and Non-Smokers Among Educated Young Adults in Visva-Bharati, Santiniketan: A Case Study
Buddhadev Ghosh
, Sukanta Nayek
and Pratap Kumar Padhy
*

1
Department of Environmental Studies,
Visva-Bharati, Santiniketan,
Birbhum,
West Bengal
India
http://dx.doi.org/10.12944/CWE.17.2.5
Copy the following to cite this article:
Ghosh B, Nayek S, Padhy P. K. Assessment of Respiratory Morbidity and Epidemiological Survey of Tobacco Smokers and Non-Smokers Among Educated Young Adults in Visva-Bharati, Santiniketan: A Case Study. Curr World Environ 2022;17(2). DOI:http://dx.doi.org/10.12944/CWE.17.2.5
Copy the following to cite this URL:
Ghosh B, Nayek S, Padhy P. K. Assessment of Respiratory Morbidity and Epidemiological Survey of Tobacco Smokers and Non-Smokers Among Educated Young Adults in Visva-Bharati, Santiniketan: A Case Study. Curr World Environ 2022;17(2).
Download article (pdf)
Citation Manager
Publish History

Introduction
The tobacco product is made from the leaves of tobacco.1,2 Tobacco leaves, after being harvested, are cured, aged, and processed in various ways.2 More than 70 tobacco plant species are known, but the chief commercial is Nicotiana tabacum (Solanaceae family).3 Tobacco contains nicotine, a prime addictive chemical, and a psychoactive (mind altering) drug that rapidly affects the central nervous system.4 Worldwide, tobacco is available in many products, including cigarettes, Bidi, pipe, chewing tobacco, and snuff or snus (a powder form inserted between the lower lip or cheek and gums).4,5 Tobacco smoke is a complex mixture of chemicals, including carbon monoxide, nicotine, phenol, polycyclic aromatic hydrocarbons (PAHs), hydrogen cyanide, benzene, formaldehyde, and tobacco-specific nitrosamines.6,7,8 About 70 chemicals are identified as carcinogenic among 7000 chemicals found in tobacco smoke.9,10 Worldwide, more than 80% of the 1.3 billion tobacco smokers are from low and middle-income countries, particularly in Asia.18 After China, India is the second-largest tobacco market globally, having about 100 million smokers.11,12 In India, 19% of men, 2% of women, and 10.7% (99.5 million) of all adults smoke tobacco.13 About 39% and 30% of Indian adults are exposed to second-hand smoking at home and workplace, respectively.13 Worldwide, with the increasing number of tobacco smokers, the death rate is also increased due to different health symptoms, such as lung cancer, change in gene expression, chronic obstructive pulmonary disease (COPD), oxidative stress, etc.14,15 The significant health risks of tobacco smokers are the brain and mental effects, less sense of smell, eye etching, teeth damage, sore throat, reduced sense of taste, cancers (lips, mouth, throat, and larynx), strokes, anxiety, respiration system damage (lung cancer, cough and sputum, shortness of breath, colds and flu, pneumonia, asthma, tuberculosis, chronic obstructive pulmonary disease, and emphysema) and other male and female reproduction diseases.1,16,17 The world is now facing one of the prevalent health crises raised by the tobacco epidemic, accounting for over 8 million deaths annually. More than 7 million deaths are caused by direct consumption of tobacco and exposure to second-hand smoke leads to a death of 1.2 million .18
Smoking directly or indirectly affects our lung function and needs frequent monitoring. Spirometric lung function test is a simple, non-invasive, reliable, and economical method widely adopted for the primary diagnosis of abnormality in lung function.19 Spirometry test is a standard lung function or pulmonary function test that measures airflow into the lungs. It estimates the breathing pattern, that is, how much air is inhaled and exhaled within the time frame. Spirometry assesses pulmonary conditions such as asthma, chronic obstructive pulmonary disease (COPD), lung fibrosis, and cystic fibrosis. India is a youth-populated nation, having almost 34% population in the age group of 15-34 years.37 The growing number of young smokers will have substantial future public health implications. With these views, the present study was conducted to ascertain the respiratory health status of educated young adult smokers and non-smokers.
Materials and Methods
Protocols and sampling
The survey was conducted randomly through personal interviews with a pre-framed questionnaire and screening related to the objectives of our study. The pre-set questions of IUATLD (International Union against Tuberculosis and Lung disease) were adopted to gain information about the individual’s respiratory health. Some more questions relevant to the study objective were also framed and standardized (SM). The study was undertaken during the period July 2018 to May 2019. Based on the smoking practices, candidates were categorized into two groups, i.e., smokers (smoking continuously for a minimum of one year) and non-smokers. The questions about smoking adoption, daily smoking behaviour, care during smoking, disposal of the smoking materials, smoking expenditure, and problematic respiratory symptoms were asked to the smokers. After that, a comparative lung function test (LFT) of the selected smokers and non-smokers was conducted using a PC-based spirometer (Model: Nano, Medikro Oy, Finland) to know their lung performances. For lung function test, various spirometric indices are measured i.e., forced vital capacity (FVC, the total volume of air can forcefully exhale from the lungs after deepest inhalation), forced expiratory volume in one second (FEV1, is defined the what volume of air expired in one second after an utmost inhalation), percentage forced expiratory volume in one second (FEV1%, is represent the FEV1/FVC ration in percentage, that can be exhaled in one second) and peak expiratory flow rate (PEFR, is an individual's highest speed of exhalation, used to monitor an individual's ability to breathe out air). Before performing the lung function test (LFT), the following criteria were maintained:
- Not tightly clothed during the test.
- Not take a hefty meal within two hours prior to the test.
- No strenuous work before the test.
- Last smoking was at least one hour before the test.
- No alcohol consumption at least four hours before the test.
- No vigorous exercise before 30 min of the test.
Upholding all the above-mentioned criteria, an individual for the LFT was selected. The present study was conducted among young adult undergraduate, postgraduate, and research scholars (age group 18 to 30) male students of different academic departments in Visva-Bharati, Santiniketan, West Bengal, India. The survey was done on 521 individuals to obtain respiratory information. Among 521 individuals, 248 (47.6%) were identified as smokers, and 273 (52.4%) were non-smokers. A spirometric lung function test (LFT) was possible to conduct among 196 (79.03%) smokers and 217 (79.49%) non-smokers.
Statistical analysis
The descriptive statistical analysis was performed to get the means, standard deviation, and frequency percentage; the odds ratio was calculated to measure the association between smokers and non-smokers health outcomes. The t-test was performed to compare means with control variables, and two-way ANOVA was executed to find out the possible effects of independent variables, body mass index (BMI) [A1] (underweight, normal, overweight, and obese) and smoking status (smokers, non-smokers) on different spirometric indices (dependent variable). The statistical analyses were carried out by SPSS ver.20 and Microsoft Excel 2010.
Results
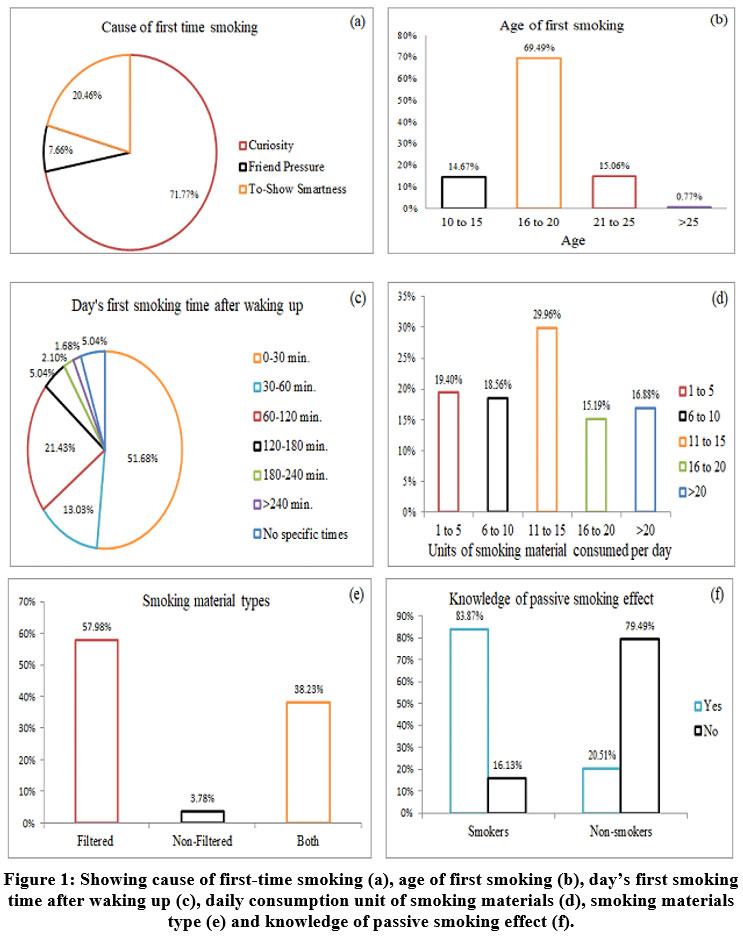
The main reason behind life’s first-time smoking was ‘curiosity,’ covering about 72% of smokers who started smoking due to this category and followed by ‘to show smartness’ was the reason in 20.46% of smokers (Fig. 1a). About 70% of the smokers started their first-time smoking at the age of 16 to 20 (Fig. 1b). 51.68% of smokers consume their day’s first smoke within half an hour after waking up in the morning (Fig. 1c). A notable smoking pattern was found between the early smokers (day’s first smoking within 30 min) and the late smokers (day’s first smoking after 30 min). Smoking patterns indicated that most early smokers were heavy smokers (smoking >10 units), which is the marker of addiction. Whereas the late smokers were not identified as heavy smokers. Among the heavy smokers, about 48% smoked 11 to 15 units per day, 24% smoked 15 to 20 units per day, and 27% smoked more than 20 units per day (Fig. 1d). About 58% of smokers used filtered smoking units (cigarette), about 4% of smokers used non-filtered smoke units (Bidi), whereas, 38% of consumers were both filtered and non-filtered user (Fig. 1e). Among the surveyed populations, about 84% of smokers knew the effect of their non-smokers passive smoking. In contrast, only 21% of non-smokers understand the impact of passive smoking (Fig. 1f).
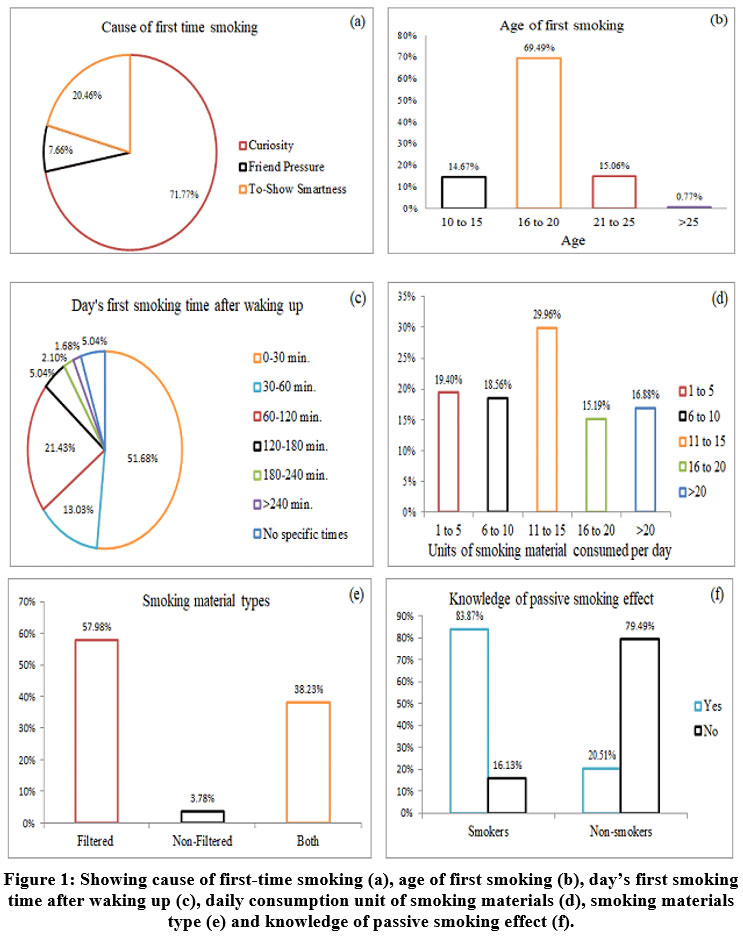 | Figure 1: Showing cause of first-time smoking (a), age of first smoking (b), day’s first smoking time after waking up (c), daily consumption unit of smoking materials (d), smoking materials type (e) and knowledge of passive smoking effect (f).
|
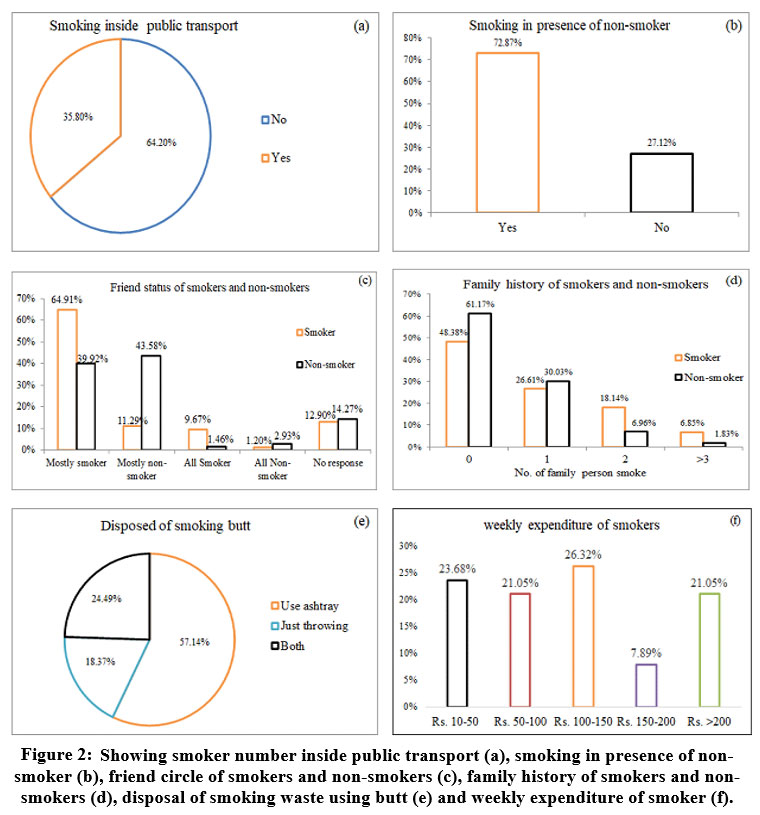
Showing social responsibility during commuting, about 64% of smokers did not smoke on public transport (Fig. 2a). But, when smokers were associated with their non-smoker friends, about 73% of smokers did not show their social responsibility to avoid smoking there (Fig. 2b). In this survey, we noticed that about 40% of the non-smoker’s population have smoker friends. Only 11% of the smoker community have friendships with non-smoker individuals (Fig. 2c). When outlining the family history of smoking, about 61% of non-smokers and 48% of smokers belonged to the ‘no smoking’ family (Fig. 2d). About 57% of smokers used ash-tray for disposing of smoked ash and butts, whereas about 18% of smokers just threw the waste carelessly (Fig. 2e). The weekly expenditure for the smoking materials varied from INR 10 to >200 rupees among the smokers. About 26%, 24%, and 21% of smokers spent an amount of INR 100 to 150, 10 to 50, and >200 weekly, respectively (Fig. 2f).
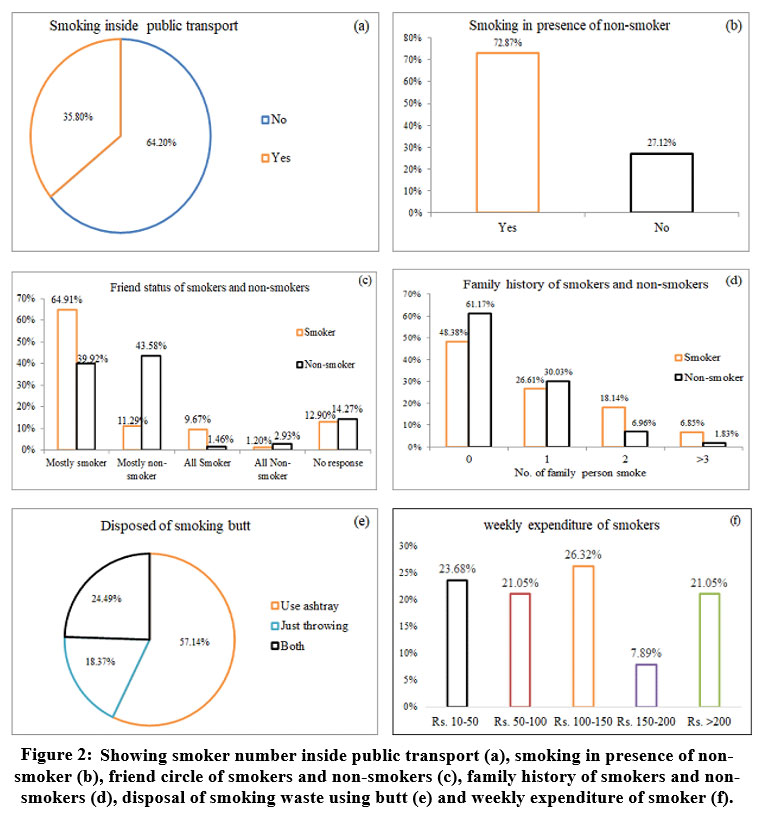 | Figure 2: Showing smoker number inside public transport (a), smoking in presence of non-smoker (b), friend circle of smokers and non-smokers (c), family history of smokers and non-smokers (d), disposal of smoking waste using butt (e) and weekly expenditure of smoker (f).
|
Anthropometric data on BMI showed that 43.54% of smokers and 32.97% of non-smokers were at risk (Table 1).
Table 1: Anthropometry of smokers and non-smokers with risk co-morbidity.
Classification | Body Mass Index (BMI) | Smokers (%) | Non- Smokers (%) | Risk of co-morbidity |
Underweight | <18.5 | 11.29 | 9.89 | Low (But increase risk of other clinical problems) |
Normal range | 18.5-22.9 | 56.45 | 67.03 | Average |
Overweight (?23) |
|
|
|
|
At risk | 23 - 24.9 | 17.74 | 13.19 | Increase |
Obese 1 | 25 – 29.9 | 13.30 | 9.52 | Moderate |
Obese 2 | > 30 | 1.21 | 0.37 | Severe |
The Asia-Pacific perspective: redefining obesity and its treatment.20
Among non-respiratory symptoms, chest pain, allergic skin, and itchiness of the eyes were common issues in smokers and non-smokers. The odds ratio (OR) of the respiratory symptoms like wheezing breath (OR = 3.8603), sore throat (OR = 2.1534), waking due to night cough (OR = 3.2436), and morning phlegm (OR = 4.4167) varied significantly in smokers as compared to non-smokers (Table 2).
Table 2: Prevalence of non-respiratory and respiratory health symptoms in young adults.
Symptoms | Smokers (%) | Non-Smokers (%) | Odds Ratio (95% CI) | Z- statistics | Significance (p) |
Frequent sneezing | 52.63 | 67.28 | 0.68 (0.43 to 1.08) | 1.639 | 0.1013 |
Nose irritation and watering | 31.57 | 42.99 | 1.15 (0.69 to 1.89) | 0.536 | 0.5921 |
Wheezing breath | 13.15 | 6.54 | 3.86 (1.74 to 8.54) | 3.333 | 0.0009 |
Sore throat | 26.31 | 18.69 | 2.15 (1.17 to 3.94) | 2.484 | 0.0130 |
Shortness of breath after heavy exercise | 21.05 | 17.76 | 1.23 (0.49 to 3.11) | 0.45 | 0.65 |
Awaking due to night cough | 26.32 | 22.43 | 3.24(1.82 to 5.76) | 4.010 | 0.0001 |
Morning phlegm | 18.42 | 11.21 | 4.41(1.9 to 10.10) | 3.522 | 0.0004 |
[CI - Confidence Interval]
In the spirometric lung function test (LFT), the mean tidal volume remained the same for both smokers (0.72± 0.28) and non-smokers (0.72 ± 0.35). Mean values of spirometric parameters like of FVC, FEV1, FEV1%, and PEFR were slightly higher in non-smokers than in smokers (Table 3). LFT revealed that 25.23%, 28.03%, and 18.03% of non-smokers were underperforming, and 26.32%, 28.95%, and 21.05% of smokers were underperforming than the predicted scores FVC, FEV1, and FEV1% respectively (Table 4). Two-way ANOVA analysis showed a non-significant effect of independent variables, BMI and smoking status on spirometric indexes. Pairwise comparison among different BMI status groups showed a significant difference of FEV1% only between normal and overweight individuals.
Table 3: Smokers and non-smokers’ spirometry mean and standard deviation with the significance level.
Parameters | Non-Smokers (Mean ± SD) | Smokers (Mean ± SD) | Significance level |
TV [Liters] | 0.72 ± 0.35 | 0.72± 0.28 | 0.946 |
FVC [Liters] | 3.83 ± 0.45 | 3.81± 0.44 | 0.725 |
FEV1 [Liters] | 3.21 ± 0.43 | 3.17 ± 0.41 | 0.579 |
FEV1/FVC [%] | 82.73 ± 8.20 | 82.01 ± 7.88 | 0.635 |
PEFR [Liters/Second] | 6.90 ± 1.44 | 6.73 ± 1.01 | 0.420 |
[SD – Standard Deviation]
Table 4: Reduction of performances based on spirometry indices.
Reduced parameters | Non-Smokers (%) | Smokers (%) |
FVC | 25.23 | 26.32 |
FEV1 | 28.03 | 28.95 |
FEV1/FVC% | 18.03 | 21.05 |
Discussion
Compulsive smoking of the senior family members in front of the children affects their health by passive smoke and creates a curiosity in their tender minds about tobacco smoking. Parental smoking influences them to adopt early life smoking by pretending to be mature. Curiosity and peer pressure are the leading causes behind the early adoption of tobacco, as found in this and other studies.21,22,23 Curiosity was reported to be the most common cause of starting smoking, followed by peer smoking.24 About 70% of smokers began their first-time smoking at the age of 16 to 20. Studies from general Indian students showed that most of them first smoked at 10 to 20 years of age.25,26,13 Family history of smoking is a well-known fact for early life initial of smoking.27,28,29,30 Consumption of the day’s first smoke within half an hour after waking in the morning was a habit in 51.68% of smokers. According to Singh et al. (2015),31 42% of Indian students feel the urge to smoke just after waking up in the morning. The urge of early smoke is associated with the risks of physical and psychological problems. Smoking just after waking up is an addictive behaviour or symptom called nicotine craving38 Smokers smoking early in the morning have a greater risk of developing lung, head, and neck cancer than other smokers.39 Smoking within 5 minutes of waking up is associated with a fourfold increase in the odds of lifetime asthma.32 In our study, about 58% of the smokers used cigarettes, which is significantly high compared to the national level of 7.3%. In contrast, about 4% of smokers used Bidi compared to the national level of 14%.13The average daily consumption of smoking materials directly affects lung function. Smoking destroys cilia, leads to a build-up of mucus in the airways, and inflammation that leads to respiratory illnesses. The airways contain air sacs called alveoli that are usually elastic.40 Smoking loses elasticity and deflates air sacs, resulting in breathing discomfort and reduced lung function capacity (inhalation and exhalation).40,41 In our study, it was found that maximum smokers consumed 11-15 units of smoking materials. According to Saha et al. (2008),33 the average daily consumption of cigarettes was 1-5 units for 41% population, followed by 6-10 units for 33% population. Passive smoking knowledge of smokers generally helps care for other non-smokers, but most smokers do not follow it. They know the health effects of smoking but could not quit it because of addiction, cheap and easy availability of smoking materials. The weekly expenditure for the smoking materials varied from 10 to >200 rupees among the smokers. In this study, 21% of young adult smokers spent about INR 700 to 800 monthly, whereas 16% of Nepali young adult student smokers spent about INR 1100 to 1200 34 Investing more than -INR 700 monthly by students is wasting enough money on the Indian scenario. In India, the total attributable costs were INR 1773.4 billion from 2017 to 2018 for treating all diseases and deaths due to tobacco smoking for persons 35 years or older. The economic costs of tobacco use amount to approximately 1% of India’s gross domestic product (GDP).42
The smokers showed their social responsibility in public places and transport by not smoking inside. The odds ratio (OR) of the respiratory symptoms like wheezing breath, sore throat, waking due to night cough, and morning phlegm varied significantly to smokers compared to non-smokers. That indicates that smokers are more susceptible to health issues than non-smokers.
The spirometry index values of TV, FVC, FEV1, FEV1/FVC, and PEFR declined in the smoker group compared to the non-smokers, indicating a better lung performance in the non-smokers group. Gold et al. (1996)35 found that FEV1/FVC decreased among adolescent smokers. The declination in pulmonary function parameters among smokers indicated that smoking is responsible for compromised lung function.36
Conclusion
This study on the smoking behaviour of educated young adults revealed that ‘curiosity,’ ‘showing smartness’ and ‘family history of smoking’ were the main critical factors for early adoption of smoking. Most of them started smoking at the age of 16 to 20 years. Heavy smokers smoke early in the morning, indicating their addiction. They smoke both filtered and non-filtered smoke units. Most smokers consume more than 10 cigarettes per day. Despite of knowing the harmfulness of passive smoking, most smokers smoke and did not care about their non-smoker friends. Different respiratory symptoms were significantly dominant in smokers compared to non-smokers. Spirometric lung performance of the adult smokers declined as compared to the non-smokers.
Limitations and future research of the study
The present study was mainly based on the smoking habits, causes of smoking, and their effects on lung functions of young adult male smokers' and non-smokers' in a small area. The future scope of this study would be to work in large areas among various age groups, having males and females, and comparing their smoking habits, causes of smoking, and lung function variations.
Acknowledgment
All authors gratefully express their heartiest thanks and acknowledge the cooperation of the young adults who participated in this study.
Conflict of Interest
There are no conflicts of interest for any author.
Funding Sources
The authors received no financial support for this research.
References
- Eriksen, M. P., Mackay, J., & Ross, H. The tobacco atlas. Atlanta, GA: American Cancer Society, 2012; 72.
- NIH, 2020. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/tobacco Accessed on 10/07/20.
- Seraji, R. A. N., Navaey, H. N., Ali, S. O., & Eslami, H. Evaluating resistance to drought stress in flue-cured tobacco varieties via stress susceptibility indexes in dry farming conditions. International Journal of Farming and Allied Sciences, 2014; 3(4), 373-376.
- West, R. Tobacco smoking: Health impact, prevalence, correlates and interventions. Psychology & health, 2017; 32(8): 1018-1036. https://doi.org/10.1080/08870446.2017.1325890.
- Walters, S. 4.2 Altering Consciousness With Psychoactive Drugs. Psychology-1st Canadian Edition, 2020.
- Kufe, D. W., Pollock, R. E., Weichselbaum, R. R., Bast, R. C. J., Gansler, T. S., & Holland, J. F. Frei El, editors. Cancer Medicine. Canada, Hamilton: BC Decker Inc., 2003.
- Rodgman, A., & Perfetti, T. A. The chemical components of tobacco and tobacco smoke. CRC press, 2013.
- Münzel, T., Hahad, O., Kuntic, M., Keaney Jr, J. F., Deanfield, J. E., & Daiber, A. Effects of tobacco cigarettes, e-cigarettes, and waterpipe smoking on endothelial function and clinical outcomes. European heart journal, 2020; 41(41), 4057-4070. https://doi.org/10.1093/eurheartj/ehaa460.
- Potera, C. Outdoor smoking areas: does the science support a ban? 2013. https://doi.org/10.1289/ehp.121-a229.
- Salem, A. F., Al-Zoubi, M. S., Whitaker-Menezes, D., Martinez-Outschoorn, U. E., Lamb, R., Hulit, J., & Lisanti, M. P. Cigarette smoke metabolically promotes cancer, via autophagy and premature aging in the host stromal microenvironment. Cell Cycle, 2013; 12(5), 818-825. https://doi.org/10.4161/cc.23722.
- Giovino, G. A., Mirza, S. A., Samet, J. M., Gupta, P. C., Jarvis, M. J., Bhala, N., ... & GATS Collaborative Group. Tobacco use in 3 billion individuals from 16 countries: an analysis of nationally representative cross-sectional household surveys. The Lancet, 2012; 380(9842), 668-679. https://doi.org/10.1016/S0140-6736(12)61085-X.
- Reid, J. L., Mutti-Packer, S., Gupta, P. C., Li, Q., Yuan, J., Nargis, N., & Hammond, D. Influence of health warnings on beliefs about the health effects of cigarette smoking, in the context of an experimental study in four Asian countries. International journal of environmental research and public health, 2017; 14(8), 868. https://doi.org/10.3390/ijerph14080868.
- GATS2 (Global Adult Tobacco Survey) Fact Sheet, India 2016-17. https://www.who.int/tobacco/surveillance/survey/gats/GATS_India_201617_FactSheet.pdf Accessed on 21/05/2019.
- WHO report on the global tobacco epidemic 2015 [Online]. World Health Organization. Available: https://apps.who.int/iris/bitstream/handle/10665/178574/9789240694606_eng.pdf?sequence=1&isAllowed=y. Accessed on 21/05/2019.
- Durham, A. L., & Adcock, I. M. The relationship between COPD and lung cancer. Lung Cancer, 2015; 90(2), 121-127. https://doi.org/10.1016/j.lungcan.2015.08.017.
- Liu, Y., Pleasants, R. A., Croft, J. B., Wheaton, A. G., Heidari, K., Malarcher, A. M., ... & Strange, C. Smoking duration, respiratory symptoms, and COPD in adults aged? 45 years with a smoking history. International journal of chronic obstructive pulmonary disease, 2015; 10, 1409. doi: 10.2147/COPD.S82259.
- Tashkin, D. P., & Murray, R. P. Smoking cessation in chronic obstructive pulmonary disease. Respiratory medicine, 2009; 103(7), 963-974. https://doi.org/10.1016/j.rmed.2009.02.013.
- WHO, 2020: https://www.who.int/news-room/fact-sheets/detail/tobacco. Accessed on21/09/2020.
- Barreiro, T., & Perillo, I. An approach to interpreting spirometry. American family physician, 2004; 69(5), 1107-1114.
- World Health Organization, 2000. The Asia-Pacific perspective: redefining obesity and its treatment, https://apps.who.int/iris/bitstream/handle/10665/206936/0957708211_eng.pdf?sequence=1&isAllowed=y. Accessed on 21/05/2020.
- Almutairi, K. M. Smoking among Saudi students: a review of risk factors and early intentions of smoking. Journal of community health, 2014; 39(5), 901-907. DOI 10.1007/s10900-014-9909-8.
- Ravishankar, T. L., & Nagarajappa, R. Factors attributing to initiation of tobacco use in adolescent students of Moradabad, (UP) India. Indian journal of dental research, 2009; 20(3), 346. DOI: 10.4103/0970-9290.57382.
- Conrad, K. M., Flay, B. R., & Hill, D. Why children start smoking cigarettes: predictors of onset. British journal of addiction, 1992; 87(12), 1711-1724. https://doi.org/10.1111/j.1360-0443.1992.tb02684.x.
- ?çmeli, Ö. S., Türker, H., Gündo?u?, B., Çiftci, M., & Aka Aktürk, Ü. Behaviours and opinions of adolescent students on smoking. Tuberk Toraks, 2016; 64(3), 217-222. doi: 10.5578/tt.20925.
- Kapoor, S. K., Anand, K., & Kumar, G. Prevalence of tobacco use among school and college going adolescents of Haryana. The Indian Journal of Pediatrics, 1995; 62(4), 461-466. https://doi.org/10.1007/BF02755068.
- Chadda, R. K., & Sengupta, S. N. Tobacco use by Indian adolescents. Tobacco induced diseases, 2002; 1(2), 1-9. https://doi.org/10.1186/1617-9625-1-2-111.
- Bhojani, U. M., Elias, M. A., & Devadasan, N. Adolescents' perceptions about smokers in Karnataka, India. BMC Public Health, 2011; 11(1), 1-8. https://doi.org/10.1186/1471-2458-11-563.
- Mukherjee, A., Sinha, A., Taraphdar, P., Basu, G., & Chakrabarty, D. Tobacco abuse among school going adolescents in a rural area of West Bengal, India. Indian journal of public health, 2012; 56(4), 286. DOI: 10.4103/0019-557X.106416.
- Kodl, M. M., & Mermelstein, R. Beyond modeling: Parenting practices, parental smoking history, and adolescent cigarette smoking. Addictive behaviors, 2004; 29(1), 17-32. https://doi.org/10.1016/S0306-4603(03)00087-X.
- Kegler, M. C., Cleaver, V. L., & Yazzie-Valencia, M. An exploration of the influence of family on cigarette smoking among American Indian adolescents. Health Education Research, 2000; 15(5), 547-557. https://doi.org/10.1093/her/15.5.547.
- Singh, S. H. I. L. P. I., Dagrus, K. A. P. I. L., KARIYA, P. B., BARGALE, S., & SHAH, S. Knowledge and attitude regarding ill effects of smoking among College students. EJDTR, 2015; 4, 259-65.
- Selya, A. S., Thapa, S., & Mehta, G. Earlier smoking after waking and the risk of asthma: a cross-sectional study using NHANES data. BMC pulmonary medicine, 2018; 18(1), 1-6. https://doi.org/10.1186/s12890-018-0672-y.
- Saha, I., Paul, B., & Dey, T. K. An epidemiological study of smoking among adult males in a rural area of Hooghly district, West Bengal, India. Journal of Smoking Cessation, 2008; 3(1), 47. https://doi.org/10.1375/jsc.3.1.47.
- Sharma, A., Sharma, B., Niraula, S. R., Devkota, S., & Pradhan, P. M. S. Smoking habit among male medical and dental students of BP Koirala Institute of Health Sciences, Nepal. Kathmandu University Medical Journal, 2013; 11(1), 32-36. https://doi.org/10.3126/kumj.v11i1.11020.
- Gold, D. R., Wang, X., Wypij, D., Speizer, F. E., Ware, J. H., & Dockery, D. W. Effects of cigarette smoking on lung function in adolescent boys and girls. New England Journal of Medicine, 1996; 335(13), 931-937. DOI: 10.1056/NEJM199609263351304.
- Walter, S., & Richard, J. Longitudinal study of lung function development in a cohort of Indian medical students: interaction of respiratory allergy and smoking. Indian J Physiol Pharmacol, 1991; 35(1), 44-48.
- https://www.thehinducentre.com/multimedia/archive/03188/Youth_in_India-201_3188240a.pdf Accessed on 16/08/2022.
- Rieder A, Kunze U, Groman E, Kiefer I, Schoberberger R. Nocturnal sleep-disturbing nicotine craving: a newly described symptom of extreme nicotine dependence. Acta Med Austriaca. 2001;28(1):21-22. doi:10.1046/j.1563-2571.2001.01005.x.
- Gu F, Wacholder S, Kovalchik S, Panagiotou OA, Reyes-Guzman C, Freedman ND, De Matteis S, Consonni D, Bertazzi PA, Bergen AW, Landi MT. Time to smoke first morning cigarette and lung cancer in a case–control study. JNCI: Journal of the National Cancer Institute. 2014 Jun 1;106(6). https://doi.org/10.1093/jnci/dju118.
- Davis JD, Wypych TP. Cellular and functional heterogeneity of the airway epithelium. Mucosal immunology. 2021 Sep;14(5):978-90. https://doi.org/10.1038/s41385-020-00370-7.
- Tantisuwat A, Thaveeratitham P. Effects of smoking on chest expansion, lung function, and respiratory muscle strength of youths. Journal of physical therapy science. 2014;26(2):167-70. https://doi.org/10.1589/jpts.26.167.
- John RM, Sinha P, Munish VG, Tullu FT. Economic costs of diseases and deaths attributable to tobacco use in India, 2017–2018. Nicotine and Tobacco Research. 2021 Feb;23(2):294-301. https://doi.org/10.1093/ntr/ntaa154.








{kind=link}
{kind=link}