Healthcare Waste Management: The Current Issue in Menellik II Referral Hospital, Ethiopia
Desta Debalkie1
*
 and Abera Kumie2
and Abera Kumie2
1
Department of Health Service Management and Health Economics,
School of Public Health,
College of Medicine and Health Sciences,
Bahir Dar Universit,
Ethiopia
2
Department of Environmental Health,
School of Public Health,,
College of Health Sciences,
ddis Ababa University,
Ethiopia
http://dx.doi.org/10.12944/CWE.12.1.06
Healthcare wastes generated in Hospitals from medical activities have not given sufficient attention. In developing countries, healthcare wastes are still handled and disposed indiscriminately creating an immense threat to the public health and the environment. This situation is much worse in Ethiopia where there is paucity of convincing evidence about healthcare waste generation rate and management system. A crossectional study was conducted in Menellik II hospital to evaluate the healthcare waste management system. Primary data on the healthcare waste management system was collected using observational checklist. Key informant interview guide was also employed on 11 selected informants to assess waste management practice and analyzed by thematic framework. The results revealed that there was no segregation of healthcare waste by type at the point of generation and disinfection of infectious waste before disposal. The main HCW treatment and disposal mechanism was incineration using low temperature, single chamber incinerator; open burning; burring in to amputation pit and open dumping on municipal dumping site as well as on the hospital back yard. Furthermore, there was negligence, attitudinal problem and low level of awareness about safe healthcare waste management. To diminish the risk of healthcare waste on public health and environment, a cost effective interventions include providing better medical waste management facilities, adherence to national regulatory and rising awareness of all concerned need to adopt in the hospital.
Copy the following to cite this article:
Debalkie D, Kumie A. Healthcare Waste Management: The Current Issue in Menellik II Referral Hospital, Ethiopia. Curr World Environ 2017;12(1). DOI:http://dx.doi.org/10.12944/CWE.12.1.06
Copy the following to cite this URL:
Debalkie D, Kumie A. Healthcare Waste Management: The Current Issue in Menellik II Referral Hospital, Ethiopia. Curr World Environ 2017;12(1). Available from: http://www.cwejournal.org/?p=16859
Download article (pdf)
Citation Manager
Publish History
Introduction
Hospital could be a place of almighty, an area to serve the patient. Since starting, the hospitals are legendary for the treatment of sick persons. However we are unaware the concerned the adverse effects of the rubbish and filth generated by them on land and atmosphere.1 The last century witnessed the fast mushrooming of hospital within the public and private sector, set by the requirements of increasing population combined with the arrival and acceptance of “disposable materials” as a result rising incidence of HIV, hepatitis, ebola etc has created the bulk generation of healthcare waste a major concern and agenda about current situation.2,3
Healthcare waste includes all wastes generated in the course of healthcare activities in the health institution: diagnosis, treatment or immunization of both human beings and animals.4 Healthcare facilities such as hospitals, research laboratories, medical and dental clinics, nursing homes, ambulance, mortuary and autopsy centers, etc. produce the tremendous amount healthcare waste containing a large component (75-90%) of general healthcare waste, which does not pose any risk to public health or the environment if properly disposed1,4-6 is comparable to municipal solid waste and a smaller portion (10-25%) of hazardous waste.1 These HCW generated as a byproduct of treating patients contained infectious, bio-medical and chemical materials are the second dangerous after radiation wastes in the world causing infections, infertility, hormonally triggered cancers, genital deformities and neurological disorders both in the short and long-term exposure if not properly disposed.5,7-9
Improper waste management generally results in adverse effects on the environment and the public health.5 Numerous studies have reported that the inappropriate handling and disposal of HCW poses risks to health workers who may be directly exposed and people near health facilities, particularly children and scavengers who make a living of recycling materials from open dump sites accessed to infectious waste specially sharps waste which had higher risk of diseases like hepatitis and HIV/AIDS.5,10-12 The World Health Organization (WHO) estimated that unsterilized syringes caused between 8 to 16 million cases of hepatitis B, 2.3 to 4.7 million cases of hepatitis C, and 80,000 to 160,000 cases of HIV infections every year.1,13 The 5.2 million people in the world including 4 million children die each year from waste management related diseases.5
Majority of the healthcare facilities (HCFs) in developing countries suffer a variety of deprivations of healthcare waste management (HCWM) system from point of generation up to the final disposal. Huge amount of healthcare wastes deposited openly in waste dumping site together with municipal domestic non-hazardous solid waste indiscriminately.14
The management of healthcare waste in many developing countries has a high concern because of the risk to the public health and the environment as a result of the implementation of improper healthcare waste management and poor data recording concerning generation rate.15
Observation regarding the practices of healthcare waste management indicated that most of the health facilities had not put in place an organized management system to address healthcare waste management properly.16,17 This was true where the case medical waste was handled like any other municipal waste in many urban settings of Ethiopia.16,18-20 Public healthcare facilities that are increasing from time to time in the city were not established with standardized buildings and infrastructures for safe treatment and disposal of wastes.
Most of the time it is disposed of in crude public dumps such as “Queshie” site in Addis Ababa and other solid waste left un collected in the city dumped by generators everywhere in their premises and vacant space.18,20 Proper handling of waste during storage, transportation, treatment and disposal is therefore important for the promotion of public health.3,5
In Ethiopia there was rapid opening of healthcare facilities in response to MDG goals and population growth which results in massive generation of HCW. However the management of healthcare waste which was given less attention by healthcare providers, managers and decision makers at hospitals in Addis Ababa city was improper resulting in percentage increase of the generation of hazardous HCW which far from UN report is poisonous to the public health and environment.14,20
Issue of HCW generation rate which was inadequately studied in Ethiopia is one of the major reasons for inadequate and improper healthcare waste management.15 Thus, there is need to assess the current situation of the healthcare waste management system and the main objective of this study was therefore, to evaluate healthcare waste management practice in Menelik II referral hospital, Ethiopia. The information generated from this is envisaged to enable policy makers, program designers and health workers to improve healthcare waste management systems and hence improve infection prevention and control at healthcare facilities in Ethiopia.
Methods and Materials
Study Characteristics
A cross-sectional qualitative study was conducted to evaluate the HCW management system in Menellik II referral hospital, Addis Ababa City from February 17 to 24, 2015. The city is the capital of Ethiopia as well as head quarter of African Union. There are 6 public hospitals under the city Administration Health Bureau that provide service for more than 3,384,569 people.21 The hospital was opened in 1909 which has now 29 active specialized case teams with 199 numbers of beds.
The study was conducted on Menellik II referral hospital selected purposively because it is the only hospital providing forensic pathology in the country and has largest number of beds as well as staff, assuming increased rate of waste generation. A similar assumption was also followed by Haylamicheal et al. (2011).
Data collection tools and procedures
To evaluate the management practice, all sources of healthcare waste case teams as well as the hospital compound in where waste was temporally stored, treated and disposed off were observed and inspected using check list. A total of 11 key informant interviews were also conducted with the officer in charge of the facility and selected workers using semi-structured interview guide to provide an understanding of the healthcare waste management culture of the facility.
Data quality assurance and analysis
Data quality was assured by relating all questions and checklist logically to the variables measured. The tool was designed to measure all components of the variables and also adapt an existing instrument that was already tested in other studies. A content analysis of the data from key informant interviews and observation were analyzed using thematic framework manually by categorizing and organizing according to thematic similarities and differences to understand relationships in the overall context of the study.
Ethical consideration
Ethical approval and clearance was obtained from School of Public Health, Addis Ababa University. Written permission for data collection was taken from Addis Ababa City Administration Health Bureau and hospital administration. All respondents were informed about the study procedures and the interview was conducted after obtaining their informed consent. The participants were assured of the confidentiality as they participate in the study.
Results
Healthcare waste segregation practice
The use of a color coding system for HCW containers (black, yellow, red, and blue) was practiced without labeling. However ,there was no segregation of HCW in to waste categories to the available color coded waste containers at the point of generation except the sharp waste made at puncture proof safety box. The municipal garbage tank contained all mixture of waste was over full and droppings of refuse around the surrounding because of delay in offsite transportation service to the municipal disposal area (Figure 1).
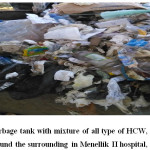 | Figure 1: Municipal garbage tank with mixture of all type of HCW, over full and droppings of refuse around the surrounding in Menellik II hospital, February 2015. Click here to View figure |
Interim storage on point of source
All case teams temporarily stored wastes in cleanable and closed dust bins. In most OPDs (especially ophthalmology, orthopedic), minor OR and food catering, the waste was stored for over 48 hrs without being treated while in EOPD and major OR stay only for 8 hours and all IPDs for 24 hours (Figure 2). All HCW categories sent to the facility dedicated place of onsite storage (municipal garbage tank capacity of 8 m3) mixing together in a manner potential to infection and hazard (Figure 1).
Healthcare waste handling, collection and transportation
In most studying case teams, HCW was collected daily at the morning except the major operating room and EOPD made within average of 8 hours. Most of the devices used for on-site transportation of HCW were closed bin with wheel. The waste on municipal garbage tank (totally infectious) was stored for minimum of a week and maximum of three weeks and transported by out sourced private company in to the city municipal disposal site “qoshe” unsanitary landfill site for open dumping. HCW bin put in the walkway and pedestrian was not emptied and clean daily (Figure 2).
 | Figure 2: HCW interim(primary) storage and transportation materials of Menellik II hospital, February 2015. Click here to View figure |
Healthcare waste recycling and reusing
Healthcare waste minimization at the source of generation, reusing and recycling was not employed by any of the case teams except recycling of plastic water bottles, film developer, reuse of packs, and suction tubes (Figure 3). Lack of commitment to initiate a recycling program was therefore the main factor of HCWM.
 | Figure 3: Water bottle plastics stored for recycling dispersed near the incinerator open field in Menellik II Hospital, February 2015. Click here to View figure |
Healthcare waste treatment and disposal
Disinfection of waste before disposal, waste storage and collection utilities was non-existent always. The main treatment and disposal mechanism was incineration, open burning; burring in to amputation pit and open dumping on municipal dumping site as well as on the hospital back yard (Figure:4-7). The hospital has functional low combustion, single chamber incinerator incinerating all type of the wastes together without separating especially general waste (Figure-5). The incinerator was made of bricks, reinforced concert slab and had air inlets for facilitation of combustion. The incinerator has relatively smaller chimney to its size, the door for the waste feeding opening had broken and no door for ash removal. There was no separate incinerator for sharps waste or needle pit. The incinerator was unable to burn waste completely; consequently the waste volume was not reduced significantly and produced air pollutant emission. At the forensic pathology case team, highly infectious waste was treated and burned openly emitting pollutants in the atmosphere (Figure-4). The pathological waste was buried into amputation pit with secured cover (Figure 7A). Furthermore, the hospital was not in compliance with applicable regulations such as prohibiting open burning, open dumping and malpractice of segregation of HCW etc.
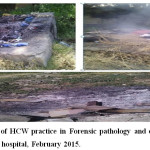 | Figure 4: Open burning of HCW practice in Forensic pathology and orthopedic ward case teams in Menellik II hospital, February 2015. Click here to View figure |
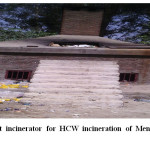 | Figure 5: A newly built incinerator for HCW incineration of Menellik II Hospital, February 2015. Click here to View figure |
 | Figure 6: Open dumping of HCW at the back yard of the Hospital, February, 2015. Click here to View figure |
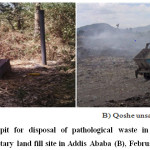 | Figure 7: Amputation pit for disposal of pathological waste in Menellik II hospital (A) and “Qoshe” unsanitary land fill site in Addis Ababa (B), February 2015. Click here to View figure |
Responsibilities, budget allocation and training on HCWM
The responsibility of HCW management was left only for the waste handlers and sanitarians in the facility. In service training about healthcare waste management was given for smaller number of staffs (63 support staff including waste handlers and 25 technical workers). HCWM regulations as well as any applicable facility based policy and strategy were not found. There was HCWM committee and HCWM guideline in the study health facility developed by ministry of health
Healthcare waste handling and processing practice (process flow of HCWM)
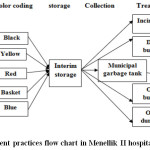 | Figure 8: Waste management practices flow chart in Menellik II hospital, February 2015 Click here to View figure |
Healthcare Waste Risk and Occupational health Safety
All staffs had information about HAI occurred as a result of malpractice of HCWM. The hospital gave HVB vaccine of 3 doses to all staff and provides all the necessary protective devices except boots and goggle. However, it was observed that some workers were not wearing while handling HCW. As a result, 13 workers had sharps and needle stick injuries in the past 6 months. There was no allocation of safety precautions like material safety data sheet for employees and people. The open burning and incomplete combustion of non segregated HCW that had PVC content at the yards of the facility was a potential to emit pollutant gases that attack the human organ.
Challenges of HCWM in the hospital
The main problems encountered in management of HCW in the study institution were low awareness, negligence and carelessness of the health workers, cleaners and patients. Poor commitment of the managerial personnel, bad attitude of health professionals in the segregation and disinfection of HCW, the resistance to wear protective gears and staff turnover were among the major one encountered.
Discussion
Most healthcare facilities in developing countries do not adequately segregate infectious or hazardous waste from ordinary domestic waste stream, the total quantity of waste classified as infectious and thus needing special handling and treatment.2-4 HCW must be appropriately labeled and segregated from the facility where it is generated to the point of treatment and disposal. Segregation which is the hallmark of HCWM offers protection to workers and the environment as well as reduces the cost of disposal.22,23
In the study hospital, different colored bags have been provided but segregation of HCW at site of origin was not implemented satisfactorily and this causes a lot of problems for the people dealing with the final disposal. This was because of weak commitment, staff attitude as well as negligence. Therefore the authorities must claim strict instructions given to the doctors and nurses involved in the generations. This was also reported in the same way by study conducted in Hawassa city that 67% of the HCFs did not segregate waste at source.14-16,24,25 This showing that implementation of healthcare waste management system is not given much priority and emphasis in the country. It is also due to inadequate orientation of auxiliary health workers. For example, research carried out on risk perception of healthcare workers towards healthcare waste management in Ethiopia showed that only a small proportion of healthcare workers adequately perceived the health risk of handling waste materials.26 This deficiency is linked with inadequate training and supervision of health workers and, lack of enforceable health regulations aimed at providing a safe waste handling and disposal.
All of the case teams in Menellik II hospital used safety boxes for collection of sharps waste. This was in line with what was reported by Debere et al 14. It was also better than the study done by Hailemicheal et al, Hawassa city, 67% of the HCFs did not use safety boxes for sharps.16 This variation may be due to difference in supply of safety boxes that is considerable in amount in government facilities than privet one. The risk of used needles and sharps injury associated with improper collection might be given better attention by governmental health system and other non-governmental supporters to reduce the transmission of HIV and other related disease, as shown by Azage et al7 and increased risk perception of sharps waste among workers in the hospital as supported by a study conducted in Gondar.26
Different studies showed in developing countries that the data available related to sharps and needle stick injury was very few and under estimation of the real risks.7 This might be true in the study hospital that sharps and needle stick injury was observed only on 13 workers within last six months even if the waste generated in the hospital is a heterogeneous mixture including sharps, needles, pathological, radiological, chemical etc which is very difficult to handle. The most important issue related to this fewer and under estimate needle stick injury is also that the hospital segregated its sharps & needles waste in an relatively proper manner. These sharps & needles are the commonest vehicle and contribute to spread of serious diseases like hepatitis, human immunodeficiency virus etc.27,28 The study by WHO strengthen this idea that unsterilized syringes cause 8 to 16 million cases of hepatitis B, 2.3 to 4.7 million cases of hepatitis C, and 80,000 to 160,000 cases of HIV every year.1,13 Five point two million People in the world (including 4 million children) also die each year from waste-related diseases.5
The way HCW transported in the hospital was better than Hawassa city facilities which used open plastic containers without wheel from the site of generation to the treatment area. In contrast to this relationship both types of waste (infectious and non-infectious) were also collected and transported once a day in the morning in most case teams in lesser regularity as compared to the Hawassa city that seven of the HCFs collect waste twice a day whereas the other two conduct collections three to four times a day.16 This was in agreement to the WHO recommendation of storage of HCW in warm climate for a maximum 48 hours during the cool season and maximum 24 hours during the hot season.9,29
In the studied hospital, the main available treatment and final disposal mechanism of HCW was incineration using low combustion, single chamber incinerator made of bricks & reinforced concrete, open burning, burring in the pit and open dumping. This was similarly reported by MMIS project of HCFs in Ethiopia: open burning in a dug hole 54%, low-temperature incineration 52% and open-air burning 18%.30 It was also supported by a study conducted in hospitals of Addis Ababa city (2012) that 83 % of the hospitals treat their HCW using low to medium combustion incinerators. The study in hospitals of two regions Ilala and Kinodoni in Tanzania showed that 70 % of HCFs in Ilala burn wastes in poorly designed incinerators and open pit while in Kinodoni 83 % of the facilities bury wastes in the pits.31 The reason behind may be lack of elaborated, legal policy and institutional framework that enables obligations & enforcement in installing standardized facilities for safe HCWM. These inadequate and sub-standard HCW facilities are also against Stockholm, Basel and Rotterdam Conventions stating that the treatment and disposal of HCW does not cause harm to human health and the environment.32 Such defective type of facilities are also associated with several problems have been reported specifically with single chamber brick-made incinerators, including emission of toxic substances into the environment that are a risk to public health.33,34 Therefore, there is a need for alternative solutions, such as De Montfort incinerator as used in Zimbabwe35 as well as installation of irradiation, encapsulation and chemical disinfection.17
A study in Tanzania indicated that about 60 % in Ilala and 70% Kinondoni municipalities surveyed HCFs incinerators were not fenced. 50% of them being of low capacity with some parts missing as well as 9 and 47% of the healthcare facilities in Ilala and Kinondoni, respectively; do not have the standard operating procedures for incineration of HCW31 was supported what actually present in Menellik II hospital that the incinerator without fence worked polluting the environment, equipped with no ash pit, broken waste loading cover, no ash removing doors and sufficient air-inlets for complete combustion of HCW. This low combustion single-chamber incinerator which may release pollutant gasses: Dioxin, furans, heavy metal and acidic gasses was against the Stockholm convection on persistent organic pollutants (POPs).17,32
In addition to having the infrastructures for safe management of HCW, it is important to raise the awareness and built attitude of healthcare workers and waste handlers. Various studies have shown that raising awareness plays an essential role in proper HCW handling and management with simple and low-cost approaches.26,36 The present study revealed the main challenge of HCWM was staff turnover, staff attitudinal problem, negligence, absence of training, and low level of awareness of safe HCWM practices by both health professionals and support staff. Therefore ensuring training of the health care workers, advocating universal safety precautions like hand washing, wearing PPE and disinfection of wastes have been proposed to bridge the existing gap. This study was not without limitations. There might be observer bias during the assessment of HCW management system, although much effort is done to minimize it. The study also did not consider generation rate; so it is suggested that future research should focus on estimation of generation rate assisted with management practice at varies seasons of the year by considering ownership and random sampling method.
Conclusion
The generation of waste should be estimated for proper management. The segregation, collection, transportation and disposal of HCW is not being implemented properly as per the standards & norms in the studied hospital there for, the health care waste leaving from the hospital as a whole is both potentially infectious and hazardous to the environment and public health in particular. This is in contribution of workers less commitment, attitudinal problems and negligence as a result of absence of adequate refreshment training for capacity building as well as poor supervision by administrators. Thus, the waste should be classified according to their source, typology and risk factors associated with their handling, storage and ultimate disposal. The waste categorization should be standardized and minimized for the convenience of its handling and cost reduction incurred by the hospital in terms of treatment and disposal. The wastes were collected and transported in most case teams using somewhat standard non labeled bins in spite of absence of separation practice. The main treatment and disposal method was incineration in to low combustion single chamber incinerator, open burning and open dumping. This low temperature incinerator is responsible for incomplete combustion and insignificant in volume reduction of waste. In such practice there is great potential to emit toxic pollutants from incineration to the atmosphere. An improved incinerator that has devices for the control of combustion should be encouraged. All in all, there is no a comprehensive healthcare waste management plan in the facility which is the key ingredient to a successful waste management. There for it is urgent to plan about HCWM essential to target and involve all the stakeholders: policy makers, hospital administrators, and health care personnel to ensure the safe handling and disposal of HCW waste, and thus preserve human health and limit environmental degradation.
Acknowledgment
The authors acknowledge the financial support from Addis Ababa University for the completion of the study. More appreciations go to Menellik II Health Science College for providing digital weighting scale of the study. The authors further thank the management of the Addis Ababa City Government Health Bureau, the hospital staff and chief executive officer for their unreserved cooperation during data collection. Finally, we extend our heartfelt thanks to the study participants, supervisor, and data collectors, where, without their participation this will not be realized.
Reference
- Healthcare without harm. Best practices in health care waste management examples from four Philippine hospitals (February 2007).
- Ahmed, N. O., Gasmelseed, G. A. & Musa, A. E. Assessment of Medical Solid Waste Management in Khartoum State Hospitals. Journal of Applied and Industrial Sciences 2 201-205 (2014).
- IPEN study groups. Bio-medical waste management: situational analysis & predictors of performances in 25 districts across 20 Indian states. Indian J Med Res 141-153 (January 2014)..
- Tabasi, R. & Marthandan, G. Clinical Waste Management: A Review on Important Factors in Clinical Waste Generation Rate International Journal of Science and Technology 3, 194-200 (March 2013).
- Akter, N. Medical Waste Management: A Review. 1-25 (January, 2000).
- UN. The adverse effects of the movement and dumping of toxic and dangerous products and wastes on the enjoyment of human rights, Calin Georgescu. (4 July 2011).
- Azage, M. & Kumie, A. Healthcare waste generation and its management system: the case of health centers in West Gojjam Zone, Amhara Region, Ethiopia. Ethiop J Health Dev 24, 120-126 (2010).
CrossRef - Kumar, R. et al. Assessment of health care waste management practices and knowledge among health care workers working at tertiary care setting of Pakistan J Health Res 27, 233-236 (August 2013).
- Chartier, Y. et al. Safe management of wastes from health-care activities. Second edition. Geneva, Switzerland, World Health Organazation. (2014).
- Titto, E. d., Savino, A. A. & Townend, W. K. Healthcare waste management: the current issues in developing countries. Waste Management & Research 30, 559-561, doi:10.1177/0734242X12447999 (2012).
CrossRef - Thakur, V. & Ramesh, A. Healthcare waste management research: A structured analysis and review (2005–2014) Waste Management & Research 33, 855-870, doi:10.1177/0734242X15594248 (2015).
CrossRef - Silva, C. E. D., Hoppe, A. E., Ravanello, M. M. & Mello, N. Medical wastes management in the south of Brazil Waste Management 25 600-605, doi:0.1016/j.wasman.2004.03.002 (14 May 2004).
- Emmanuel, J. Eighth international waste management congress and exhibition. (June 2007)
- Debere, M. K., Gelaye, a. A., Alamdo, A. G. & Trifa, Z. M. Assessment of the health care waste generation rates and its management system in hospitals ofAddis Ababa, Ethiopia, 2011. BMC Public Health 13, 1-9 (2013).
CrossRef - Tesfahun, E., Abera Kumie, Legesse, W., Kloos, H. & Beyene, A. Assessment of composition and generation rate of healthcare wastes in selected public and private. Waste Management & Research 32, 215-220, doi:10.1177/0734242X14521683 (3 February2014).
CrossRef - Haylamicheal, I. D., Dalvie, M. A., Yirsaw, B. D. & Zegeye, H. A. Assessing the management of healthcare waste in Hawassa city, Ethiopia. Waste Management & Research 29, 854-862, doi:0.1177/0734242X10379496 (2011).
- Ndidi, N., Nelson, O., Patricia, O. & Sunday, J. Waste management in healthcare establishments within Jos Metropolis, Nigeria African Journal of Environmental Science and Technology 3, 459-465, doi:10.5897/AJEST09.119 (December, 2009 ).
- Tadesse, T. Solid and hazardous waste wanagement lecture notes for Environmental Health science students. (August 2004).
- Tulu, F. D.Hazardous waste management by healthcare institutions, addis ababa: implementation of laws and regulation. Ethiopian Journal of Environmental Studies & Management 7, 134 - 141, doi::http://dx.doi.org/10.4314/ejesm.v7i2.4 (February 19, 2014).
CrossRef - Desta, H., Worku, H. & Fetene, A. Assessment of the contemporary municipal solid waste management in urban environment: The case of Addis Ababa, Ethiopia. Journal of environmental science and technology 7, 107-122 (2014).
- EDRE Population Census Commission. Summary and statistical report of the 2007 population and housing census population size by age and sex. (Deceber 2008)..
CrossRef - Col A.K. Jindal, Y., Gupta, S. L. C. A., Grewal, L. C. V. S. & Mahen, A. C. A. Biomedical waste disposal: A systems analysis. Medical journal armed forces India a 6 9 (201 3)351e356351-356 (2013).
- Nema, A., Pathak, A., Bajaj, P., Singh, H. & Kumar, S. A case study: biomedical waste management practices at city hospital in Himachal Pradesh Waste Management & Research 29 669-673, doi:10.1177/0734242X10396753 (2011).
CrossRef - Farzadkia, M., Moradi, A. & Mohammadi, M. S. Hospital waste management status in Iran: a case study in the teaching hospitals of Iran University of Medical Sciences. Waste Management & Research 27, 384-389, doi:10.1177/0734242X09335703 (2009).
CrossRef - Tadesse, M. L. & Kumie, A. Healthcare waste generation and management practice in government health centers of Addis Ababa, Ethiopia. BMC Public Health 14, 1221, doi:10.1186/1471-2458-14-1221 (2014).
CrossRef - Yenesew, M. A., Moges, H. G. & Woldeyohannes, M. A cross sectional study on factors associated with risk perception of healthcare workers toward healthcare waste management in health care facilities of Gondar Town, Northwest Ethiopia. Int J Infect Control, 8, 1-9, doi:10.3396/ijic.v8i3.024.12 (2012.).
CrossRef - FMOH. Infection prevantion and patient safety reference for service providers and managers in healthcar facilities of Ethiopia second edition . (Feb 2012).
- Thakur, V. & Ramesh, A. Healthcare waste management research: A structured analysis and review (2005–2014) Waste Management & Research 33, 855-870, doi:10.1177/0734242X15594248 (2015).
CrossRef - FEPA. Technical guidline on the environmentally sound managent of biomedical and healthcare waste , Addis Ababa Ethiopia (2004).
- FMOH. Assessment of cealth care waste management status in health facilities of Ethiopia (Addis Ababa, Ethiopia, February 2006).
- Manyele, S. V. & Lyasenga, T. J. Factors affecting medical waste management in low level health facilities in Tanzania. African Journal of Environmental Science and Technology 4, 304-318 (May 2010).
- FDRE House of People Representatives. a proclamation to ratify the stockholm convention on persistent organic pollutants vol. 279/2002 1767. Federal Negarit Gazeta, Ethiopiaj (July 2002)
- M, Z. & Shareefdeen. Medical Waste Management and Control. Journal of Environmental Protection 3, 1625-1628 (November 26th, 2012).
CrossRef - Odette, R. H. et al. Assessment of healthcare waste generation and its management systems: A prevalence survey of the healthcare facilities in Madagascar. Journal of Environmental Science, Toxicology and Food Technology 8, 20-29 (July 2014).
CrossRef - WHO, African Region Harrare, Zimbabwe. Managing health care waste disposal: guidelines on how to construct, use, and maintain a waste disposal unit.(February 2005).
- Kapoor, D., Nirola, A., Kapoor, V. & Gambhir, R.-S. Knowledge and awareness regarding biomedical waste management in dental teaching institutions in India- A systematic review. J Clin Exp Dent 6, 19-24, doi:10.4317/jced. 51565 (2014;6(4):e419-24.).







